POST ABORTION HUMAN FETAL
HARVESTING
TABLE OF CONTENTS
A. THE NATURE OF AND TRADITIONAL TREATMENT FOR PARKINSON’S DISEASE
B. HARVESTED FETAL BRAIN TISSUE TRANSPLANTS FOR PARKINSON’S DISEASE
C. WHAT THIS PAPER WILL EXAMINE
D. SELECTED HUMAN FETAL ANATOMY & BEHAVIOR MILESTONES
-1ST TRIMESTER
-2ND TRIMESTER
-3RD TRIMESTER
E. SELECTED METHODS OF ABORTION
-SUCTION (VACUUM ASPIRATION) ABORTION
-DILATATION & CURETTAGE (D&C) ABORTION
-SALT POISONING ABORTION
-HYSTEROTOMY ABORTION
-DILATION & EXTRACTION (D&X); aka PARTIAL BIRTH ABORTION
-RU-486 ABORTION
-DILATATION & EVACUATION (D&E) ABORTION
-PROSTOGLANDIN ABORTION
-INDUCED LABOUR ABORTION aka LIVE BIRTH ABORTION
F. SELECTED FETAL RESPONSES TO ABORTION
-A 12-WEEK FETUS REACTS TO A SUCTION ABORTION
-21+ WEEK GESTATION BABIES [DURING] LIVE BIRTH ABORTION
-ABORTED FETUS CASES DELIVERED LIVE TO A FETAL HARVESTING LAB TECHNICIAN BY
ABORTION DOCTORS
-A 26 WEEK FETUS RESPONDS TO PARTIAL BIRTH ABORTION
G. THE FETAL HARVESTING INDUSTRY
-THE FETAL HARVESTING FIRMS
-A THRIVING AND PROFITABLE INDUSTRY
-HOW THE US FETAL HARVESTING INDUSTRY OPERATES
-THE CUSTOMERS OF US FETAL HARVESTING FIRMS
-HARVESTED FETAL “DONORS” MUST BE IN OPTIMAL CONDITION
-LATE TERM FETAL “DONORS” NOT UNCOMMON
-WHAT FETAL HARVESTING FIRMS MARKET
-FRESH FETAL “DONORS” MOST DESIRED
H. CONCLUSIONS
I. REFERENCES (with working internet links)
A. THE NATURE OF AND TRADITIONAL TREATMENT FOR PARKINSON’S DISEASE:
Carleson, in “Physiology of Behavior” (8th edition) describes the cause of
Parkinson’s disease and its current standard drug treatment as follows (page
117):
“Degeneration of dopamiergic neurons that connect the substantia nigra with
the caudate nucleus causes Parkinson’s disease, a movement disorder
characterized by tremors, rigidity of the limbs, poor balance, and a
difficulty in initiating movements. The cell bodies of these neurons are
located in a region of the brain called the substantia nigra…” (1)
“People with Parkinson’s disease are given L-DOPA, the precursor to
dopamine. Although dopamine cannot cross the blood-brain-barrier, L-DOPA
can. Once L-DOPA reaches the brain, it is taken up by dopaminergic neurons
in patients with Parkinson’s disease. As a consequence, the patient’s
symptoms are alleviated.” (1)
The same source notes the complications of and limitations of treating
Parkinson’s disease with L-DOPA (page 265):
However, treatment of Parkinson’s disease with L-DOPA “often produces
dyskinesias and dystonias - involuntary movements and postures that are
presumably caused by too much stimulation of dopamine receptors in the basal
ganglia… In addition, L-DOPA does not work indefinitely; eventually, the
number of nigrostriatal dopaminergic neurons declines to such a low level
that the symptoms become worse. Some patients… even become bedridden,
scarcely able to move.” (1)
B. HARVESTED FETAL BRAIN TISSUE TRANSPLANTS FOR PARKINSON’S DISEASE:
Carlson in the same “Physiology of Behavior” then reports briefly on one
possibly promising long term treatment for Parkinson’s disease involving the
injection of harvested fetal brain tissue into the brains of patients with
Parkinson’s disease (page 265):
“…Transplantation of fetal tissue attempts to reestablish the secretion of
dopamine in the neostriatum. The tissue is obtained from the substantia
nigra of aborted human fetuses and implanted into the caudate nucleus and
putamen by means of stereotaxically guided needles…. Scans have shown that
dopaminergic fetal cells are able to grow in their new host and secrete
dopamine, reducing the patient’s symptoms. “ (1)
C. WHAT THIS PAPER WILL EXAMINE
The therapy of implanting harvested post abortion fetal brain tissue into
the brains of Parkinson’s disease patients raises interesting questions that
are not covered by Carlson in his “Physiology of Behavior” textbook. The
Text takes one from a 28 day old human embryo as a “neural tube” to a living
and thriving post birth human infant while remaining curiously silent on the
intervening in utero period. (1) What are the bio-psychological milestones of
human fetal development? What are the different types of abortion
procedures? How does the human fetus respond to abortion? What is the nature
of fetal harvesting? This paper will attempt to address these questions.
D. SELECTED HUMAN FETAL ANATOMICAL and BEHAVIORAL MILESTONES:
1st TRIMESTER
@ 18 days:
***Eyes start to develop. (2)
@ 20 days:
***Foundations of brain, spinal cord and nervous system are laid. (2)
@ 24 days:
***Heart begins to beat. (2)
@ 28 days:
***Muscles are developing along the future spine. Arms and legs are budding.
(2)
@ 30 days:
***Brain has human proportions. (2)
@ 35 days:
***Pituitary gland in brain is forming. Mouth, ears and nose are taking
shape. (2)
@ 6-7 weeks:
***Brain coordinates movement of muscles and organs. Reflex responses have
begun. (2)
***Brain waves detected. (2,3,4)
@ 8 weeks:
***“…the neuro-anatomic structures are present…. [a] a sensory nerve to feel
the pain and send a message to [b] the thalamus… and [c] motor nerves that
send a message to that area… The pain impulse goes to the thalamus. It sends
a signal down the motor nerves to pull away from the hurt.” (5)
***Sticking the fetus in the palm of the hand with a sharp object causes him
to open his mouth and pull his hand away. (5)
***Lip tactile response may be evoked (2,5)
***Spontaneous movements have begun. (2,3,6)
***Taste buds are forming. (2)
***Steady heartbeat heard with an ultrasound stethoscope. (7)
@ 9 weeks:
***Eyelids are sensitive to touch. (2)
***Child will bend fingers around an object placed in the palm. (2,7)
***Thumb sucking occurs. (2,8)
@ 10 weeks:
***Body is sensitive to touch. Child squints, swallows, puckers up brow and
frowns. (2,4)
***More body movement observed, such as jumping. (8)
@ 11 weeks:
***Face and the upper and lower extremities are sensitive to touch. (5)
***Makes some facial expressions, such as smiling. (2)
***Makes a fist. (4)
@ 12 weeks:
***Squinting is observed. (7)
***Draws knees up to the chest. Kicking begins. (2,9)
***Arms wiggle and head moves. (9)
***Leaps about in uterus. (6)
PICTURE/LINK:
@ 10 weeks
gestation - IN UTERO LIVE. 10-Weeks Ultrasound. AbortionFacts.com

PICTURE/LINK:
@ 9
weeks gestation - ABORTED DEAD. First Trimester [Abortion] Photographs.
AbortionTV.com

2nd TRIMESTER
@ 13 weeks:
***Vigorous fetal activity is observed: the child can kick, turn feet, curl
and fan toes, make a fist, move thumbs, bend wrists, turn head, open mouth,
press lips tightly together, jump and wave arms. (2,10)
***Breathing is practiced. (2)
@ 14 weeks:
***Most body surfaces are sensitive to pain. (5)
***Delicate finger movements present. (6)
@ 16 weeks:
***Child grasps with hands, swims and turns somersaults, fan toes, vigorous
moving and kicking. Thumb sucking observed. (2,7)
***Child hears and reacts to external sounds: Classical music has a calming
effect, while hard rock music has an agitating effect on the child. (7)
@ 18 weeks:
***Mother first feels baby's movements. (2)
@ 20 weeks:
***Clear sleep patterns evident. (2,7)
***A slamming door will provoke activity. (2)
***Child scratches himself. (7)
***Mother senses punching, kicking and elbowing by child on a regular basis.
(7)
***Vocal cords now functional and used to cry. (7)
***Yawning begins. (6)
@ 21 weeks:
***Child documented during fetal surgery via hysterotomy to reach out of
mother’s uterus and grasp surgeon’s finger with vigorous hand grasp. (11)
***Babies borne alive at this premature age can survive, but require
intensive care. (12)
@ 24 weeks:
***Child sticks out tongue. (13)
PICTURE/LINK:
@ 21 weeks gestation - POST DELIVERY LIVE.
@ 21 weeks gestation - IN
UTERO DURING SURGERY LIVE. Samuel’s Spina Bifida Surgery In Utero. Michael
Clancy.
__________________________________________________________
3rd TRIMESTER
@ 7 months:
***Eyelids blink. (2,7,6)
***Eyes look around. (2,7)
***Hands grasp is strong. (2,7)
***Child recognizes mother‘s voice from others. (2,7)
***Mother aware when child hiccups. (7)
@ 8 months:
***Child senses difference between light and darkness through mother’s
abdomen. (7)
***Taste taste-buds functional; child prefers sweet to sour. (7)
***Smiling, frowning, yawning and swallowing observed. (7)
@ 9 months:
***The now fully formed & developed child triggers labor and birth occurs,
usually 255-275 days after conception. (27)
PICTURE/LINK:
@ 30 weeks gestation - ABORTED DEAD.
Right and Wrong Made Simple.

E. SELECTED METHODS OF ABORTION:
“Abortion is the medically induced, premature death of a pre-born baby in
the womb.” (14) Abortion may be accomplished by any one or combination of
methods:
SUCTION (VACUUM ASPIRATION) ABORTION
The cervix is stretched to allow passage of a hollow suction tube into the
pregnant uterus, which has sharp-edged openings near its tip. Powerful
suction force is then applied, allowing the fetus to be ripped apart into
pieces that are then suctioned out of the uterus into a collection
container. The placenta is then suctioned out from the uterus. In post-12
weeks pregnancy terminations, supplemental instruments are often required to
crush and remove fetal parts that are too large to be evacuated by suction.
Most 1st trimester abortions in North America and the United Kingdom are
done in this manner. (15,16,17)
PICTURE/LINK:
@ 10 weeks gestation - ABORTED DEAD. Abortion by Vacuum Aspiration.

DILATATION and CURETTAGE (D and C) ABORTION
A surgical procedure that can serve to abort a 1st trimester fetus. The
cervix is dilated and a curette - a sharp loop-bladed knife - is inserted
into the pregnant uterus in order to cut the fetus and placenta into pieces.
The dismembered fetal parts and related tissue are then scraped out of the
womb into a basin. The fetal remains must then be accounted for to assure
all relevant tissues have been removed from the mother. This technique is
often associated with significant maternal bleeding. (18,16,17)
PICTURE/LINK:
@ estimate 2nd trimester - ABORTED DEAD. Abortion by Dilation and Curettage.
Society for the Protection of Unborn
SALT POISONING ABORTION
Used after 16 weeks, this technique is no longer used commonly in western
nations, but is employed often in third world nations because of its cost
effectiveness and ease of administration. A syringe of a concentrated salt
solution is injected into the amniotic fluid via a long needle through the
mother’s abdomen. The fetus then breathes and swallows the hyper-salted
amniotic fluid. The fetus struggles and sometimes seizes until dead within
usually one hour. The mother typically then delivers a dead fetus within one
to two days. The complication of fetal survival upon delivery is not
uncommon. The fetal skin upon delivery, having been chemically burned away
by the hyper-salted amniotic fluid, usually presents as a glazed red
surface. This abortion procedure was first developed in Nazi concentration
camps during World War II. (21,16,17)
PICTURE/LINK:
@ estimate late 2nd trimester or early 3rd trimester - ABORTED DEAD.
Abortion by Salt Poisoning.

HYSTEROTOMY ABORTION
Used for late term abortions in rare instances. Identical to a Caesarian
Section delivery used to deliver a live baby in the presence of certain
pregnancy/fetal complications, except the object here is to deliver a dead
fetus. A low abdominal incision is made into the pregnant uterus. If the
fetus is alive, the complication of delivering a live baby is to be avoided.
The live fetus is first terminated while still in the mother’s womb, such as
by cutting of the umbilical cord. Once the fetus is dead, the fetus is then
physically lifted out of the mother’s womb and the abortion is completed.
(22,16)
PICTURE/LINK:
@ estimate early 3rd trimester - CAESARIAN SECTION DELIVERY LIVE (?) OR
HYSTEROTOMY ABORTION DEAD (?) Abortion by Hysterotomy.

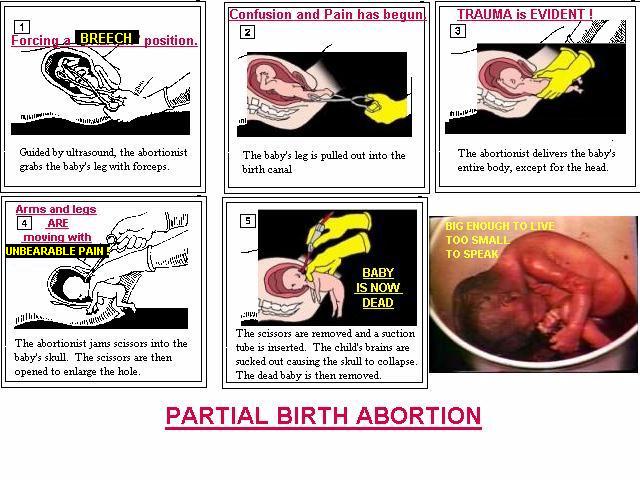
DILATION and EXTRACTION (D and X); aka PARTIAL BIRTH ABORTION
Used in well developed 2nd and 3rd trimester pregnancies. The cervix is
dilated over a period of time. The fetus is located via ultrasound, which
serves to guide the entrance of forceps into the mother’s womb. A foot is
grasped and the fetus is placed into a face-down breech (feet first)
delivery position. The fetus is then pulled out of the uterus, but keeping
the head still inside the mother’s cervix. Surgical scissors are then
inserted into the skull at the back of the neck and an opening is thus
enlarged to allow placement of a large-bore suction catheter attached to
high powered suction. The fetal brain is then suctioned out of the fetal
cranial vault. The fetus is now dead and the delivery is completed.
(19,20,16,21,17)
PICTURE/LINK:
@ estimate
mid to late 3rd trimester gestation - ABORTED DEAD. Partial Birth Abortion.
Save My Children Ministry.
RU-486 ABORTION
An early pregnancy abortion inducing drug containing Methotrexate taken
after the mother misses her period. The drug blocks the use of an essential
substance by a newly implanted fetus, causing fetal death and then
separation from the uterine wall. The dead fetus and associated tissues are
then passed vaginally by the mother. No longer able to induce abortion after
six to eight weeks of pregnancy. (16)
DILATATION & EVACUATION (D and E) ABORTION
Used for 2nd trimester abortions, at which point in fetal development the
fetal bones become calcified. A pliers-like instrument is inserted through
the dilated cervix into the pregnant uterus. Fetal body parts are grasped
and twisted off from the fetal body one at a time and removed from the
uterus. It may be necessary to snap the fetal spine and crush the fetal
skull to remove them through the dilated cervix. Fetal body parts must be
“reassembled” to assure that all fetal tissue has been removed from the
mother’s womb. (16,17)
PROSTOGLANDIN ABORTION
Used to abort mid and later term pregnancies. The hormone prostoglandin is
administered to the pregnant mother, such as via injection into the amniotic
fluid and vaginal suppositories. The hormone induces violent premature labor
contractions, thus expelling the fetus. The fetus usually dies in the
process of delivery, but the complication of live fetal birth is not
uncommon. To avoid this complication, drugs lethal to the fetus are often
injected into the amniotic fluid, thus assuring fetal death before delivery.
(23,16,17)
INDUCED LABOUR ABORTION ( aka LIVE BIRTH ABORTION)
Premature delivery of a commonly midterm fetus is induced via various means,
the objective being to deliver a premature baby that is not capable of
surviving outside the uterus. When such abortions typically produce the
complication of live birth, the now delivered living baby is provided only
“comfort care“ - wrapping the infant in a blanket - and denied all medical
and nursing care. Such infants can linger for hours before dying of “natural
causes.” (24)
F. SELECTED FETAL RESPONSES TO ABORTION: A 12-WEEK FETUS REACTS TO A SUCTION ABORTION
Dr. Bernard Nathan son - a former abortionist - narrates the video, “The
Silent Scream:” a real time fetal ultrasound video of a live 12-week fetus
undergoing a suction abortion:
Part 6 “The clip begins with an ultrasound of the fetus (girl) who is about
to be aborted. The girl is moving in the womb; …and is at times sucking her
thumb. As the abortionist’s suction tip begins to invade the womb, the child
rears and moves violently in an attempt to avoid the instrument. Her mouth
is visibly open…” (25)
Part 7 “The child’s heart rate speeds up dramatically…[as the suction
catheter makes contact with the fetus]. She moves violently away in
an]…attempt to escape the instrument….” (25)
In an article in the London Telegraph on 8/28/2000 titled “British Medical
Experts Say Unborn Children Feel Pain During Abortion,” Dr. and Mrs. J. C.
Wilke, comment on the abortion video “The Silent Scream” [above]:
“…What of The Silent Scream? A Real-time ultrasound video tape and movie of
a 12- week suction abortion is commercially available as, The Silent Scream,
narrated by Dr. B. Nathanson, a former abortionist. It dramatically, but
factually, shows the pre-born baby dodging the suction instrument time after
time, while its heartbeat doubles in rate. When finally caught, its body
being dismembered, the baby’s mouth clearly opens wide — hence, the title…”
(26)
21-23 WEEK GESTATION BABIES UNDERGOING “LIVE BIRTH ABORTION”
Nurse Jill Stanek, RN on 7/20/2000, in testimony before a US House of
Representatives committee hearing on HR4292 - the “Born Alive Infant
Protection Act of 2000” - reported the following regarding live birth
abortion infants at a “Christ Hospital” - where she was employed as a Nurse
in the labor & delivery ward:
“The method of abortion that Christ Hospital uses is called "induced labor
abortion," also now known as "live birth abortion."… It is not uncommon for
one of these live aborted babies to linger for an hour or two or even
longer. One of them once lived for almost eight hours. In the event that a
baby is aborted alive, he or she receives no medical assessments or care but
is only given what my hospital calls "comfort care." "Comfort care" is
defined as keeping the baby warm in a blanket until he or she dies.” (24)
“One night, a nursing co-worker was taking an aborted Down's Syndrome baby
who was born alive… I cradled and rocked him for the 45 minutes that he
lived. He was 21 to 22 weeks old. He was too weak to move very much,
expending any energy he had trying to breathe…” (24)
Nurse Stanek further testified to the US House committee:
“…a patient who was 23+ weeks pregnant, and it did not look as if her baby
would be able to continue to live inside of her… But the patient chose to
abort. The baby was born alive… After delivery the baby, who showed early
signs of thriving, was merely wrapped in a blanket and kept in the Labor and
Delivery Department until she died 2-1/2 hours later.” (24)
ABORTED FETUS CASES DELIVERED ALIVE TO A FETAL HARVESTING LAB TECHNICIAN BY
ABORTION DOCTORS A 2/2000 article in Coral Ridge Ministries’ Impact Newsletter titled
“Industry for Baby Body Parts Uncovered,” reveals that aborted fetus cases
born alive are terminated by abortion doctors by various means just prior to
delivery to fetal harvesting labs on the premises of abortion clinics:
“This Frankensteinian saga surfaced when "Kelly," a fetal parts worker, told
her story in 1997 to Life Dynamics, a Texas pro-life group. After a two-year
undercover investigation, Life Dynamics went public last year with her
first-hand account, documented by copies of orders for baby body parts sent
to Planned Parenthood abortion clinics.” (27)
“…she tells how an abortionist presented her with 24-week-old twins in a
bucket. "Got you some good specimens – twins," he announced as the infants,
Kelly recalls, were "still moving and gasping for air." When Kelly refused
to end the babies' lives, the doctor obliged her by drowning them in sterile
water. (27)
“That was not the only live birth Kelly witnessed. She claimed that in
numerous instances unborn children between 16 and 30 weeks old were killed
outside the womb when a doctor broke their neck or beat them to death with
tongs…” (27)
A 26 WEEK FETUS RESPONDS TO PARTIAL BIRTH ABORTION
On 3/21/1996, Nurse Brenda Shafer, RN testified before a US House of
Representatives committee hearing on HR1833 - The Partial Birth Abortion Ban
Act. Nurse Shafer reports that she was present for three “partial birth
abortions” at an abortion clinic. She shares her observations of a 26 ½ week
fetus responding to a “partial birth abortion:”
“I am a registered nurse…In September, 1993, …assignment at the Women's
Medical Center, which is operated by Dr. Martin Haskell… I stood at a
doctor's side as he performed the partial-birth abortion procedure… I worked
as an assistant nurse at Dr. Haskell's clinic for three days-- September 28,
29, and 30, 1993…” (20)
“I was present for three of these partial-birth procedures. It is the first
one that I will describe to you in detail. The mother was six months
pregnant (26 1/2 weeks)… Dr. Haskell brought the ultrasound in and hooked it
up so that he could see the baby. On the ultrasound screen, I could see the
heart beating… As Dr. Haskell watched the baby on the ultrasound screen, the
baby's heartbeat was clearly visible on the ultrasound screen.” (20)
“Dr. Haskell went in with forceps and grabbed the baby's legs and pulled
them down into the birth canal. Then he delivered the baby's body and the
arms-- everything but the head. The doctor kept the baby's head just inside
the uterus.” (20)
“The baby's little fingers were clasping and unclasping, and his feet were
kicking. Then the doctor stuck the scissors through the back of his head,
and the baby's arms jerked out in a flinch, a startle reaction, like a baby
does when he thinks that he might fall.” The doctor opened up the scissors,
stuck a high-powered suction tube into the opening and sucked the baby's
brains out. Now the baby was completely limp… ” (20)
G. THE FETAL HARVESTING INDUSTRY:
In 1997, “Kelly” - a former fetal harvesting lab technician who worked in an
abortion clinic - reported to Life Dynamics, Inc. [a pro life group] on her
experiences in the fetal harvesting industry. Life Dynamics conducted a two
year undercover investigation and then went public with her testimony and
documented evidence of the industry in 1999. (27,28,29,30,31)
THE FETAL HARVESTING FIRMS
At least two US fetal harvesting firms have received recent media attention
- AGF (Anatomical Gift Foundation) and Opening Lines. At least one - AGF -
is set up as a non-profit organization. These firms collect, prepare and
ship harvested fetal remains from abortions. (28,29,30)
A THRIVING AND PROFITABLE INDUSTRY
Opening Lines claims in its literature to fill over 1,500 fetal parts orders
per day. (27,29) AGF had revenues of more than $2 million dollars in 1998.
(28)
HOW THE US FETAL HARVESTING INDUSTRY OPERATES
In the USA, the US Federal Uniform Anatomic Gift Act has made it illegal to
buy or sell fetal remains. (27,29) Violation of this law is a federal
felony, carrying penalties of up to 10 years in prison and $250,000 in
fines. (27)
To circumvent this law, US fetal harvesting firms are charged a “site fee”
by abortion clinics to cover the costs of allowing fetal harvest lab
technicians the use of space at US abortion clinics. The collected fetal
remains are then “donated” by the abortion clinics to the fetal harvesting
firms. These firms in turn then “donate” the desired fetal remains to
clients, who in turn “reimburse” the fetal harvesting firms for their costs
of collection and shipping. (27,28,29,30)
THE CUSTOMERS OF US FETAL HARVESTING FIRMS
Clients of US fetal harvesting firms like AGF and Opening Lines are sent
overnight to public universities, pharmaceutical firms, and private research
laboratories in the US and the world. (27,28)
HARVESTED FETAL “DONORS” MUST BE IN OPTIMAL CONDITION
Such researchers ordering harvested fetal remains make such requests as
“normal donor; healthy, no genetic disorder; healthy mother.” (27) One
former fetal harvest lab technician reported that at least 90% of the
aborted fetus subjects she saw for harvesting appeared to be healthy, “These
had to be the most perfect specimens we could give these researchers for the
best value.” (28)
LATE TERM FETAL “DONORS” NOT UNCOMMON
One fetal harvest protocol obtained by Life Dynamics from a client reads,
“Whole eyes … Fresh, remove eye with as much optic nerve intact as possible.
Whole intact Leg, include ENTIRE HIP JOINT, 22-24(-) weeks gest…. Kelly (the
same former fetal harvest lab tech) reports she harvested organs from 30 to
40 “late” term fetal subjects per week. (28)
WHAT FETAL HARVESTING FIRMS MARKET
Such fetal harvesting firms market fetal eyes, livers, spleens, pancreases,
brains, thymuses, bone marrow, cardiac blood, venous blood from limbs,
extremities, spines, spinal cords and kidneys. (27,28,29,30) Thus, one fetal
cadaver can be marketed to multiple clients for multiple orders.
One such firm - Opening Lines - markets fetal livers for $150; two fetal
limbs for $150; fetal bone marrow for $350; fetal brains for $999 (with a
30% discount if significantly fragmented). (29,27,30) AGF markets fetal
livers for $360; fetal hearts for $490; fetal spines for $630. (29)
FRESH FETAL “DONORS” MOST DESIRED
Kelly [again the same fetal harvest lab technician] reports one instance in
which a doctor at the abortion clinic where she worked delivered live fetal
subjects to her for dissection. She reports the abortion doctor walked into
the fetal harvest lab and said to her, "Got you some good specimens. Twins."
She reports the pan the doctor carried contained two perfectly formed
24-week-old babies moving and grasping for air. Kelly reports she objected
saying, "They are moving. I don’t do this. That’s not in my contract." In
response to her objection, the abortion doctor reportedly immediately filled
the pan until the mouths and noses of the fetal subjects were covered by
water. (29)
Kelly further reported this was not an isolated case, “Sometimes the fetus
appeared to be dead, but when you’d open up the chest cavity, you’d see the
heart beating… They were coming out alive…with three to four live-births in
a typical two-week period.” (28)
Documents of orders obtained from Planned Parenthood abortion clinics by
Life Dynamics confirms that clients requested fetal harvesting to be done
immediately after fetal death. Such requests stated,
“Whole eyes … Fresh, remove eye with as much optic nerve intact as possible.
Whole intact Leg, include ENTIRE HIP JOINT, 22-24(-) weeks gest…. To be
removed from fetal cadaver within 10 minutes. The tissue needs to be snap
frozen as fresh as possible.” (28)
Life Dynamics uncovered other fetal harvest protocols revealing that clients
wanted fetal remains to be collected as soon after fetal death as possible.
One request reads, "Tissue should be removed and prepared under aseptic
conditions within a maximum of ten minutes after circulation has stopped.”
(27) Another request for fetal placenta, liver, heart and lung be dissected
"ASAP (within 30 minutes)." (27)
One of Opening Line’s marketing brochures assures clients of "the freshest
tissue prepared to your specification and delivered in the quantities you
need it." (29)
H. CONCLUSIONS
This paper began in the text “Physiology of Behavior” (8th edition, 2004) by
Carlson. (1) The text discusses the long-term failure of treating
Parkinson’s disease with the drug L-DOPA - the precursor for dopamine. One
emerging possible surgical treatment involves injecting of harvested aborted
human fetal dopamine-producing brain tissue into the brains of Parkinson’s
disease patients. This raises questions about human fetal neurological
development, abortion methods, fetal behavior responses to abortion and the
fetal harvesting industry - none of which are covered in the psychobiology
text in question. We are left to ponder on our own how a neural-tube-shaped
human embryo at 28 days gestation becomes a fully formed, living human
infant some time after birth. (1) Thus this paper.
Anatomy and behaviors relevant to human fetal psychobiology in the 1st, 2nd
and 3rd trimesters were briefly listed. Selected pictures of live in utero
and aborted human fetus subjects at different ages of pregnancy were noted.
The information reviewed strongly suggests that the human fetus begins early
in gestation to show clear anatomy and behaviors that are distinctly human.
Selected methods of abortion were briefly reviewed. Several pictures of
aborted human fetus subjects were presented. This raised the very relevant
question of how the human fetus behaves in response to abortion. Commentary
on a real-time ultrasound recorded abortion of a 12-week live fetus -
narrated by a well experienced former abortion doctor - was presented. Eye
witness testimony at US Congressional hearings of two Registered Nurses -
one who witnessed “live birth abortions” and another who witnessed “partial
birth abortions” on late 2nd trimester and 3rd trimester fetus subjects was
reviewed. Accounts of aborted fetus subjects delivered still alive by
abortion doctors to fetal harvesting lab technicians at an abortion clinic
was presented. These accounts strongly suggest that human fetal subjects
undergoing abortion respond to and suffer from the termination of their
lives in a distinctly human manner.
Lastly the US fetal harvesting industry was briefly examined. Human fetal
“donors” provide tissues, organs and body parts at US abortion clinics to
industry, academic and research facilities across the nation and abroad.
Although buying and selling of fetal remains in the US is prohibited by
federal law, money changes hands between abortion providers, fetal
harvesting firms and recipients of fetal remains. Clients requesting
specific fetal remains were shown to prefer later term fetus subjects who
are screened for ideal health in which the harvesting is done immediately
after fetal death. One aborted human fetus can be marketed for multiple
fetal matter to multiple clients. Some aborted human fetal subjects are
delivered still alive post abortion at abortion clinics to fetal harvesting
labs on the premises. The marketing of aborted fetal dopamine-producing
brain tissue for treatment of Parkinson’s disease patients is but one small
submarket in this new industry. END |